Tulalip TV’s Tulalip Health Watch will air this summer and will focus on health issues Native Americans face today. Photo/ Brandi N. Montreuil, Tulalip News
TULALIP, WA – Tulalip TV viewers will soon be able to watch a new informational program called “Tulalip Health Watch,” which focuses on health issues Native Americans face today.
In the program’s first episode, “Diabetes,” the disease is examined through interviews with health professionals at the Tulalip Karen I. Fryberg Health Clinic. Viewers will learn the fundamental characteristics of diabetes, along with resources available for testing, prevention, and treatment.
Diabetes affects 57 million Americans, and only 8.3 percent are diagnosed. But more shocking are the epidemic proportions of diabetes in Indian Country with 16.2 percent Native Americans and Alaska Natives diagnosed.
According to the U.S. Department of Health and Human Services and Indian Health Service, Native Americans are at a 2.2 times higher risk than their non-Indian counterparts. Between 1994 and 2004 there was a 68 percent increase in diabetes diagnosis in American Indian and Alaska Native youth, aged 15-19 years old.
In “Diabetes,” viewers will learn how a poor diet, lack of regular exercise, and a genetic pre-disposition are the leading contributing factors for 95 percent of American Indians and Alaska Native with Type 2 diabetes, and 30 percent with pre-diabetes.
Viewers will also learn how clinic staff incorporates Tulalip culture and traditions into programs available at the clinic for diabetes education, prevention, and management.
“The providers that we have here are great. The Tribe is putting money into this clinic and our goal is to be here with an open mind and heart, and to be a partner here for them regarding their health needs. We have a collaborative team here that you don’t see at other clinics,” said Bryan Cooper, Tulalip Karen I. Fryberg Health Clinic Nurse Practitioner in “Diabetes.”
“Tulalip Health Watch,” will air this summer. Future episodes will explore heart disease, obesity, and other health issues Native Americans face.
You can watch “Tulalip Health Watch” on Tulalip TV at www.tulaliptv.com or on channel 99 on Tulalip Cable.
Brandi N. Montreuil: 360-913-5402; bmontreuil@tulaliptribes-nsn.gov
FLAGSTAFF, Ariz. (AP) – Facing a high prevalence of diabetes, many American Indian tribes are returning to their roots with community and home gardens, cooking classes that incorporate traditional foods, and running programs to encourage healthy lifestyles.
The latest effort on the Navajo Nation, the country’s largest reservation, is to use the tax system to spur people to ditch junk food.
A proposed 2 percent sales tax on chips, cookies and sodas failed Tuesday in a Tribal Council vote. But the measure still has widespread support, and advocates plan to revive it, with the hope of making the tribe one of the first governments to enact a junk-food tax.
Elected officials across the U.S. have taken aim at sugary drinks with proposed bans, size limits, tax hikes and warning labels, though their efforts have not gained widespread traction. In Mexico, lawmakers approved a junk food tax and a tax on soft drinks last year as part of that government’s campaign to fight obesity.
Navajo President Ben Shelly earlier this year vetoed measures to establish a junk-food tax and eliminate the tax on fresh fruit and vegetables. At Tuesday’s meeting, tribal lawmakers overturned the veto on the tax cut, but a vote to secure the junk-food tax fell short. Lawmakers voted 13-7 in favor of it, but the tax needed 16 votes to pass.
The Dine Community Advocacy Alliance, which led the effort, said it plans to revise the proposal and bring it before lawmakers again during the summer legislative session.
“We’re going to keep moving on it,’’ group member Gloria Begay said. “It’s not so much the tax money – it’s the message. The message being, ‘Let’s look at our health and make healthier choices.’ We have to go out and do more education awareness.’’
Shelly said he supports the proposal’s intent but questioned how the higher tax on snacks high in fat, sugar and salt would be enacted and regulated. Supporters say the tax is another tool in their fight for the health of the people.
“If we can encourage our people to make healthier choices and work on the prevention side, we increase the life span of our children, we improve their quality of life,’’ said professional golfer Notah Begay III, who is among supporters.
American Indians and Alaska Natives as a whole have the highest age-adjusted prevalence of diabetes among U.S. racial and ethnic groups, according to the American Diabetes Association. They are more than twice as likely as non-Hispanic whites to have the disease that was the fourth leading cause of death in the Navajo area from 2003 to 2005, according to the Indian Health Service.
Native children ages 10 to 19 are nine times as likely to be diagnosed with Type 2 diabetes, the IHS said.
The proposed Navajo Nation tax wouldn’t have added significantly to the price of junk food, but buying food on the reservation presents obstacles that don’t exist in most of urban America. The reservation is a vast 27,000 square miles with few grocery stores and a population with an unemployment rate of around 50 percent. Thousands of people live without electricity and have no way of storing perishable food items for too long.
“They have a tendency to purchase what’s available, and it’s not always the best food,’’ said Leslie Wheelock, director of tribal relations for the U.S. Department of Agriculture.
Wheelock said the diabetes issue in tribal communities is one that has been overlooked in the past or not taken as seriously as it could be. It has roots in the federal government taking over American Indian lands and introducing food that tribal members weren’t used to, she said.
To help remedy that, the USDA runs a program that distributes nutritional food to 276 tribes. Grants from the agency have gone toward gardening lessons for children within the Seneca Nation of Indians in New York, culturally relevant exercise programs for the Spirit Lake Tribe in North Dakota and food demonstrations using fresh fruit and vegetables on the Zuni reservations in New Mexico.
The Dine Community Advocacy Alliance estimated a junk-food tax would result in at least $1 million a year in revenue that could go toward wellness centers, community parks, walking trails and picnic grounds in Navajo communities in Utah, New Mexico and Arizona. It would have expired at the end of 2018.
No other sales tax on the Navajo Nation specifically targets the spending habits of consumers. Alcohol is sold in a few places on the reservation but isn’t taxed. Retailers and distributors pay a tobacco tax.
Opponents of the junk food tax argued it would burden customers and drive revenue off the reservation. Mike Gardner, executive director of the Arizona Beverage Association, said the lack of specifics in the legislation as to what exactly would be taxed could mean fruit juice and nutritional shakes could be lumped in the same category as sodas.
“I don’t think they mean that, but that’s what will happen,’’ Gardner said. “It’s a little loose, a little vague. It’s going to create problems for retailers and … it doesn’t solve the problem.’’
FLAGSTAFF, Ariz. — The Navajo Nation president has vetoed a proposal to impose an additional tax on chips, cookies and sweetened beverages on the country’s largest reservation, but the legislation could be resurrected later.
President Ben Shelly supports the idea of a junk food tax as a way to combat high rates of diabetes and obesity among tribal members and encourage healthy lifestyles, his adviser Deswood Tome said Wednesday. But Shelly said the legislation isn’t clear on how the tax on snacks high in fat, sugar and salt would be enforced and regulated, according to Tome.
“There are a lot of supporters out there for the tax, and again, the president wants a plan that works,” Tome said. “He’s asking the (Tribal) Council to take back this initiative and redo it so that the burden is not on the government to implement a law that is going to create hardship, especially in the collection of taxes.”
The Dine Community Advocacy Alliance and tribal lawmakers had been positioning the Navajo Nation to become the leader in Indian Country when it comes to using the tax system to press tribal members to make healthier choices.
School districts across the country have banned junk food from vending machines. Cities and states have used taxes and other financial incentives to encourage healthy choices, according to the National Conference of State Legislatures, but not all the efforts have been met with overwhelming support.
The legislation in the Navajo Nation Council did not have a smooth ride either.
Denisa Livingston of the Dine Community Advocacy Alliance said the group worked for two years to get tribal lawmakers to pass the legislation. Dine is the Navajo word for “the people.”
Livingston said American Indians are more likely to suffer from diabetes and other chronic health problems than the average American.
She estimated that imposing an additional 2 percent tax on junk food sold on the Navajo reservation would result in at least $1 million a year in revenue that could go toward wellness centers, community parks, walking trails and picnic grounds in tribal communities. The tax would have expired at the end of 2018.
“Every one of our Navajo families has someone who is suffering from chronic disease,” she said. “This is the initiative we wanted to take because we see our families suffering.”
About 14 percent of the people in the area of the Navajo Nation have been diagnosed with diabetes, according to the federal Indian Health Service.
American Indian and Alaska Native adults are twice as likely to be diagnosed with diabetes as non-Hispanic whites, and Native children ages 10 to 19 are nine times as likely to be diagnosed with type 2 diabetes, the agency said.
Opponents of the tax in Navajo communities in Arizona, New Mexico and Utah argued it would burden consumers and drive revenue off the reservation.
Shelly also vetoed a companion bill to eliminate the tribe’s 5 percent sales tax on nuts, fresh fruits and vegetables. Tome said Shelly would like lawmakers to revise the legislation to address his concerns.
The Tribal Council can override Shelly’s vetoes with a two-thirds vote of its 24 members. Livingston said she would pursue that option with lawmakers.
Read more here: http://www.theolympian.com/2014/02/12/2981159/navajo-nation-president-blocks.html#storylink=cpy
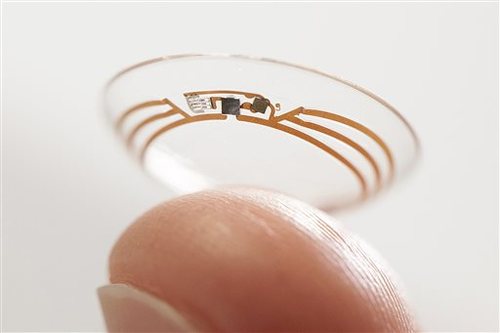
Google contact lens could be option for diabetics This undated photo released by Google shows a contact lens Google is testing to explore tear glucose. After years of scalding soldering hair-thin wires to miniaturize electronics, Brian Otis, Google X project lead, has burned his fingertips so often that he can no longer feel the tiny chips he made from scratch in Google’s Silicon Valley headquarters, a small price to pay for what he says is the smallest wireless glucose sensor that has ever been made. (AP Photo/Google)
January 16, 2014 Martha Mendoza AP
MOUNTAIN VIEW, Calif. (AP) – Brian Otis gingerly holds what looks like a typical contact lens on his index finger. Look closer. Sandwiched in this lens are two twinkling glitter-specks loaded with tens of thousands of miniaturized transistors. It’s ringed with a hair-thin antenna. Together these remarkable miniature electronics can monitor glucose levels in tears of diabetics and then wirelessly transmit them to a handheld device.
“It doesn’t look like much, but it was a crazy amount of work to get everything so very small,” he said before the project was unveiled Thursday.
During years of soldering hair-thin wires to miniaturize electronics, Otis burned his fingertips so often that he can no longer feel the tiny chips he made from scratch in Google’s Silicon Valley headquarters, a small price to pay for what he says is the smallest wireless glucose sensor ever made.
Just 35 miles away in the beach town of Santa Cruz, high school soccer coach and university senior Michael Vahradian, 21, has his own set of fingertip callouses, his from pricking himself up to 10 times a day for the past 17 years to draw blood for his glucose meter. A cellphone-sized pump on his hip that attaches to a flexible tube implanted in his stomach shoots rapid-acting insulin into his body around the clock.
“I remember at first it was really hard to make the needle sticks a habit because it hurt so much,” he said. “And there are still times I don’t want to do it _ it hurts and it’s inconvenient. When I’m hanging out with friends, heading down to the beach to body-surf or going to lunch, I have to hold everyone up to take my blood sugar.”
The idea that all of that monitoring could be going on passively, through a contact lens, is especially promising for the world’s 382 million diabetics who need insulin and keep a close watch on their blood sugar.
The prototype, which Google says will take at least five years to reach consumers, is one of several medical devices being designed by companies to make glucose monitoring for diabetic patients more convenient and less invasive than traditional finger pricks.
The contact lenses were developed during the past 18 months in the clandestine Google X lab that also came up with a driverless car, Google’s Web-surfing eyeglasses and Project Loon, a network of large balloons designed to beam the Internet to unwired places.
But research on the contact lenses began several years earlier at the University of Washington, where scientists worked under National Science Foundation funding. Until Thursday, when Google shared information about the project with The Associated Press, the work had been kept under wraps.
“You can take it to a certain level in an academic setting, but at Google we were given the latitude to invest in this project,” Otis said. “The beautiful thing is we’re leveraging all of the innovation in the semiconductor industry that was aimed at making cellphones smaller and more powerful.”
American Diabetes Association board chair Dwight Holing said he’s gratified that creative scientists are searching for solutions for people with diabetes but warned that the device must provide accurate and timely information.
“People with diabetes base very important health care decisions on the data we get from our monitors,” he said.
Other non-needle glucose monitoring systems are also in the works, including a similar contact lens by Netherlands-based NovioSense, a minuscule, flexible spring that is tucked under an eyelid. Israel-based OrSense has already tested a thumb cuff, and there have been early designs for tattoos and saliva sensors.
A wristwatch monitor was approved by the FDA in 2001, but patients said the low level electric currents pulling fluid from their skin was painful, and it was buggy.
“There are a lot of people who have big promises,” said Dr. Christopher Wilson, CEO of NovioSense. “It’s just a question of who gets to market with something that really works first.”
Palo Alto Medical Foundation endocrinologist Dr. Larry Levin said it was remarkable and important that a tech firm like Google is getting into the medical field and that he’d like to be able to offer his patients a pain-free alternative from either pricking their fingers or living with a thick needle embedded in their stomach for constant monitoring.
“Google, they’re innovative, they are up on new technologies, and also we have to be honest here, the driving force is money,” he said.
Worldwide, the glucose-monitoring devices market is expected to be more than $16 billion by the end of this year, according to analysts at Renub Research.
The Google team built the wireless chips in clean rooms and used advanced engineering to get integrated circuits and a glucose sensor into such a small space.
Researchers also had to build in a system to pull energy from incoming radio frequency waves to power the device enough to collect and transmit one glucose reading per second. The embedded electronics in the lens don’t obscure vision because they lie outside the eye’s pupil and iris.
Google is now looking for partners with experience bringing similar products to market. Google officials declined to say how many people worked on the project or how much the firm has invested in it.
Dr. David Klonoff, medical director of the diabetes research institute at Mills-Peninsula Health Services in San Mateo, worked with Google to see whether glucose is present in tears and whether the amount of glucose is proportional to the amount of glucose in blood. He’s still analyzing but optimistic about his findings and warns there are many potential pitfalls.
“Already this has some breakthrough technologies, but this is a moonshot, there are so many challenges,” he said.
One is figuring out how to correlate glucose levels in tears as compared with blood. And what happens on windy days, while chopping onions or during very sad movies? As with any medical device, it would need to be tested and proved accurate, safe, and at least as good as other types of glucose sensors available now to win FDA approval.
Karen Rose Tank, who left her career as an economist to be a health and wellness coach after her Type 1 diabetes diagnosis 18 years ago, also is encouraged that new glucose monitoring methods may be on the horizon.
“It’s really exciting that some of the big tech companies are getting into this market,” she said. “They bring so much ingenuity; they’re able to look outside the box.”
Tribal member Ron Anchetta takes home the broccoli he grew in the community garden at the health clinic.
By Andrew Gobin, Tulalip News
“Rather than making multiple appointments throughout the week, today we have made available every service for diabetes testing all at once,” said Bryan Cooper about the October 15th diabetes day at the Tulalip Karen I. Fryberg Health Clinic. A day meant to inform about the disease also offers tips on diabetes prevention, healthy living, and general nutrition.
Cooper, the medical director at the clinic, made key points as to why diabetes day is a success, such as explaining the ease of diabetes testing, both for patients and staff.
“Our labs are nationally accredited. Here at the clinic, lab results are ready in 15 minutes, which is unheard of at larger clinics and hospitals.”
Although Cooper is one of the lead organizers, he emphasized the importance of the team of specialists that make diabetes day possible. “The team made themselves available, making it possible to have integrated services to streamline diabetes testing. That was one concern we kept hearing from patients, that testing was too time consuming, spanning multiple days and appointments,” said Cooper. “Today, patients can come in and get everything done at once, and it doesn’t take long to make it through each necessary station.”
Diabetes day is one aspect of a five-year plan developed last summer to create programs at the clinic geared towards community needs. Diabetes day began January of this year, and it happens 4 times a year, to allow for the convenient service for new patients, as well as those diabetic patients that need to be seen every 3 months. The staff would really like to see the clinic become a place for the community wellness center, where people could come and relax and visit, not just for medical needs.
“In addition to dental and medical, we offer alternative medicine such as acupuncture, reiki, bowen, massage, chiropractor, and traditional healing. We have a garden of traditional foods available to patients as well,” said Cooper.
Visit the clinic to learn more about upcoming events and programs, or to learn more about any of these services provided.
Staff enjoyed a morning treat of warm whole wheat frybread. Photo by Brandi N. Monteuil
By Monica Brown, Tulalip News Writer
TULALIP, Wash.-There’s something about frybread, maybe it’s that you can smell it a mile away and that scent brings back so many memories. This recipe was received as a request to test and it was surprisingly good. Since it contains mostly whole wheat flour it offers more filling fiber, which also helps to lower the net carbs of this tasty snack. The recipe indicates that it will make eight small frybread but I was able to make just over ten.
Since it is important to having slightly fluffy frybread, be sure that your baking powder is fresh. Test it by placing a tsp. into a small cup of warm or hot water, if it bubbles up immediately then it is still fresh. If not you will either need to buy more or make your own by combining, 1 tsp baking soda, 2 tsps cream of tartar and 1 tsp of corn starch (optional). Baking soda can be tested for freshness in the same manner but by placing a tsp in a small amount of vinegar.
This recipe can be found at www.diabetes.ihs.gov in the printed materials section. If you have a recipe that you would like to share please send it in to mbrown@tulaliptribes-nsn.gov. Recipe adapted from What’s cooking, Healthy in Warm Springs, Sara Lee Thomas, MS, RD and Edison Yazzie
Whole wheat Frybread
Ingredients:
2 cups whole wheat flour
1 cup white flour
3 tablespoons powdered milk
1 tablespoon baking powder
1 teaspoon salt (optional)
1 ½ cups warm water
Canola oil
Preparation:
Mix dry ingredients in a bowl and gradually add water to make dough. Knead the dough until it forms a ball and comes clean from the edge of bowl. Cover with a cloth and let sit for 30 minutes.
Pour about ¾ inch of canola oil into a deep frying pan and heat on medium. Test the temperature of the oil by putting a small pinch of dough into it. If the oil is ready, the will rise immediately to the top.
Divide the dough and knead into 8 round balls. Pat and stretch or roll dough out into flat circles until the dough is ¼ to ½ inch thick. With a fork, poke a few holes in the flattened circles of dough.
Carefully slide a flattened dough round into the hot oil to avoid splashes. Slightly lift frybread to check the bottom, when it is begins to brown turn it over. When both sides are done remove from oil, drain excess oil and place on baking sheet lined with paper towels.
Nutrition Information Makes 8 frybread
240 calories, 10g Total fat, 1g Saturated fat, 220-510mg Sodium, 35g Carbohydrate, 4g fiber, 6g Protein
whole wheat frybread with homemade jam. Photo by Brandi N. Montreuil
ROSEBUD | Connie Brushbreaker was a 12-Coke-a-day drinker when she was diagnosed with diabetes after the birth of a child. Now, she’s helping lead an effort on the Rosebud Indian Reservation to change the mindset of Native Americans here so they no longer view the disease as an inevitable part of life.
Brushbreaker started a diabetes education program 15 years ago that soon will include a new wellness center, a mobile unit to travel around the nearly 2,000-square-mile reservation and a plan to certify diabetes educators who are American Indian. The $5.4 million investment came from Denmark-based Novo Nordisk Inc., the world’s largest manufacturer of insulin, which planned to unveil the program at a Friday ceremony in Rosebud.
“I think we’re going to be able to do wonders — to get the word out there. And if we help only a handful of people, that will save in the budget but also could save some lives,” said Brushbreaker.
American Indians and Alaska Natives have the highest age-adjusted prevalence of diabetes among U.S. racial and ethnic groups, according to the American Diabetes Association. And they are 2.2 times more likely than non-Hispanic whites to have the disease, according to the Indian Health Service. From 1994 to 2004, there was a 68 percent increase in diabetes among native youth ages 15-19 years. And an estimated 30 percent of American Indians and Alaska Natives have pre-diabetes, the diabetes association said.
Loss of eyesight and amputations are common results of the disease on the reservation, and dozens of patients require kidney dialysis, Brushbreaker said.
“Native Americans can tolerate a higher blood sugar level. They get used to it,” said Rita Brokenleg, a registered nurse for Rosebud’s program.
“Our challenge is to help people understand why this is important,” she said.
Access to affordable, nutritious food is also a problem because most people live in poverty and the choices for non-processed foods are few.
“As natives, our bodies weren’t made to process the starches. Back in the old days, we were active. We had to hunt for our food,” Brushbreaker said.
She said a lack of funding, space and staff has limited what she can do, and tribal members have asked for help.
The new wellness center, which is still under construction, will offer the types of fitness classes and education that are accessible in much of the rest of the country. The building now used for classes is too small, Brushbreaker said. The biggest room is 8 by 10 feet, which makes yoga or Zumba difficult.
Because many of the more than 21,000 tribal members on Rosebud don’t have transportation, the mobile unit will travel throughout the reservation — which is larger than the state of Rhode Island — and screen people, Brushbreaker said.
The certified native educators are needed because IHS, which provides health care to Indians, no longer has any educators on the reservation, she said.
“People come into my office because they’ve not been given any information on what’s going on with their body,” Brushbreaker said. “They’ll go in to see the doctor and they’ll say, ‘here’s medication for your diabetes’ and the patient has never been told they have diabetes.”
The American Diabetes Association, in an email to The Associated Press, said the effort should help: “Reservations may be located in remote areas with limited access to health care and exercise facilities with proper exercise equipment, so this innovative program has potential to have high impact, especially since many reservations have limited resources (financial, land, etc.). Additionally, a wellness center that emphasizes proper nutrition and provided education would be extremely beneficial to those on reservations.”
Novo Nordisk founded the World Diabetes Foundation to diagnose and help people with diabetes in developing countries. Rosebud is the first such project in North America, said the pharmaceutical company’s general counsel, Curt Oltmans, who grew up nearby in Nebraska and made meat deliveries to Rosebud while in college.
“I said if I’m ever in a position to help the people, I’d like to do that,” Oltmans said by phone from Princeton, N.J. “Almost 30 years later, I had this opportunity to get involved.”
Details of the program will be presented in December at a conference in Melbourne, Australia, at the World Diabetes Congress, he said.
“My personal hope is that this is going to lead better awareness and education and screening on the reservation. We have a fear that there’s a lot of undiagnosed diabetes,” Oltmans said. “Their views are very Third World, unfortunately, uninformed views of diabetes.”
The Rosebud program is drawing attention from other groups that work with Native Americans, and the company views it as a long-term commitment, Oltmans said.
“A lot of companies say, ‘Here’s your mobile unit and wellness center, good luck,'” he said. “We’re going to have to stay engaged. We’re going to measure. Are we having an impact? How many people go to the wellness center? What are their ages? Are they losing weight? Are their numbers getting better or are they getting worse?”
Wellness Center and Mobile Medical Unit Boost Education and Screening Efforts through Partnership with Novo Nordisk
Novo Nordisk, Aug 23, 2013
ROSEBUD, SD, August 23, 2013 – Addressing one of the biggest health problems facing Native American communities everywhere, the Rosebud Sioux Tribe today unveiled a new, state-of-the-art wellness center and a first-of-its kind mobile diabetes medical unit. These resources will allow the Rosebud Sioux Tribe Diabetes Prevention Program (RSTDPP) to improve screening and intervention in children, as well as promote healthy lifestyles for people of all ages on the reservation. The center and mobile unit were made possible through funding from global healthcare company Novo Nordisk as part of its Native American Health Initiative.
“Diabetes is a serious problem for my tribe, but we know we can turn it around,” said RSTDPP Director Connie Brushbreaker. “Education and screening can help raise awareness about diabetes. The wellness center and mobile unit are smart ways to help us reach more people on our reservation and provide valuable disease education.”
Overall, American Indian and Alaska Native adults are more than twice as likely to have diagnosed diabetes compared with non-Hispanic whites.[1] In some American Indian/Alaska Native communities, diabetes prevalence among adults is as high as 60%.[2]
The new wellness center will house exercise facilities, diabetes education and nutrition training space, and exam rooms. The facility will also provide secure storage for the mobile medical unit, which can travel to the remote corners of the reservation to promote diabetes education, screening and prevention to residents that have limited access to care.
The enhanced diabetes prevention and screening efforts were recommended as part of a thorough, four-month assessment of the diabetes care and educational programs currently available to residents of Rosebud by the internationally-recognized Park Nicollet International Diabetes Center, a nonprofit diabetes care, education, and clinical research facility based in Minneapolis, Minnesota.
“This program has several important components to addressing diabetes in Indian country,” said Donald K. Warne, MD, MPH, professor at North Dakota State University and advisor to the project. “One of the most important issues is making an early diagnosis before complications start to occur. Too often, once a diagnosis is made there are barriers to accessing medical care, so bringing professional medical services to people through a mobile unit is both innovative and essential to improving quality of care.”
The initial investment of $3 million from Novo Nordisk also enables the formation of a diabetes education program for healthcare professionals and patients, the implementation of a community awareness initiative for diabetes prevention, and the creation of scholarships through the support of the American Association of Diabetes Educators that will allow tribe members to be trained as certified diabetes educators.
Curt Oltmans, corporate vice president and general counsel at Novo Nordisk, grew up near the Rosebud Reservation and witnessed the disparities in care facing the Native American population first-hand. He is leading Novo Nordisk’s Native American Health Initiative.
“For more than three years Novo Nordisk has engaged with the Rosebud Sioux Tribe to design this initiative,” Oltmans said. “As a leader in diabetes, we believe that diabetes education and prevention are essential. Our Diabetes Educators have trained the community’s health representatives and members of the Diabetes Prevention Program. It has been a privilege for our employees to learn about the tribe’s traditions and culture. We are committed to the program and we want it to become a model for others.”
The Rosebud Sioux Tribe, a branch of the Lakota people, is located on the Rosebud Indian Reservation in south central South Dakota. The federally recognized Indian tribe has more than 31,000 enrolled members and over 11,300 individuals currently residing on the reservation and its lands. The reservation has a total area of 1,442 square miles, while the total land area and trust lands of the reservation cover 5,961 square miles. The reservation includes all of Todd County, S.D. and extensive lands in four adjacent counties. The tribal headquarters is in Rosebud, S.D. For more information, visit www.rosebudsiouxtribe-nsn.gov.
[1] Source: American Diabetes Association, Native American Complications (http://www.diabetes.org/living-with-diabetes/complications/native-americans.html)
[2] Source: Special Diabetes Program for Indians Overview, May 2012 (http://www.ihs.gov/MedicalPrograms/Diabetes/HomeDocs/Resources/FactSheets/2012/Fact_Sheet_SDPI_508c.pdf)
– See more at: http://www.noodls.com/view/559834ED9E32BB3F409145101A8FDB17D6EB63FD#sthash.6L0U3kz4.dpuf
The Tulalip diabetes team is pleased to provide an opportunity for receiving a wide range of diabetic services at one time. Our team is dedicated to assisting you with improving your health thru education, healthy foods, screenings and by having activities available for you to enjoy. If you have access to our services at the health clinic, please arrange to come anytime from 9-1pm. We will have breakfast and snacks available plus some quality incentive items for your participation.
If you have diabetes and are on Medicare, you have an important decision to make in less than one month.
You have probably heard that Medicare is changing the system through which you get your diabetes testing supplies. So unlike now, when you can order supplies from thousands of mail order companies, beginning July 1 you’ll only be able to order from 18.
There is little question that this new system will be better in the long run. The government will save money and you will see your co-pay and deductible amounts decrease. For example, patients testing one time a day, before July 1, have an average co-pay of approximately $14.47 on their testing supplies. After July 1, for the same order, the co-pay will decrease to approximately $4.49. This is a savings to you of almost 70%! The actual cost may be even lower or no cost at all if you have secondary insurance.
Yet despite these significant benefits, in the short term this new system is causing confusion for patients who must change providers. They don’t know where to begin. And this makes them vulnerable to scammers who might see an opportunity to trick patients into giving personal information.
At Diabetes Care Club, we have heard these types of concerns from people who call searching for a new provider. They are rightly apprehensive about moving to another company and don’t know exactly what questions to ask.
Patients wonder what matters most when choosing a provider. And, of course, the answer to that question depends on what the patient values most. Still, after years in the diabetes care industry, I believe there are some key points that patients and their caregivers should consider before selecting a provider to trust with their healthcare needs.
How much experience does the provider have? A provider should have a proven record of excellence in distributing diabetes supplies and responding to large numbers of customers. If you receive a call or email from a provider and are unsure of their legitimacy, it is important to check your sources before providing any personal information. Medicare will not call patients about this change so if you receive a call claiming to be from Medicare, it is a scam.
Is the provider big enough to handle more customers without disruption? A provider should be able to explain in detail how it has prepared to take on thousands of new customers beginning on July 1.
Is diabetes the provider’s main focus? Ideally, a provider should make diabetes care its top priority rather than spreading its resources over a range of medical issues.
What ordering options does the provider offer? A provider should allow patients to order testing supplies by phone, email, or online and offer convenient hours for customer support.
Does the provider accept “assignment?” All mail-order providers must accept assignment, which means they cannot charge more than the prices set by Medicare. But retail outlets like pharmacies do not have to accept assignment and can charge more. It is important to ask to make sure you are not paying added costs.
What products does the provider stock? A quality provider should offer a wide range of products so that patients can get a product that best meets their needs.
Does the provider handle all the paperwork? A quality provider will handle any paperwork associated with Medicare, saving patients time and effort with these confusing forms.
Does the provider deliver on time and for free? Patients should expect their provider to cover the costs of shipping and guarantee that testing supplies will arrive on time and in proper condition.
I also recommend that patients and their caregivers visit www.NationalDiabetesSupplyFinder.com, a website that helps people find the names of all 18 providers authorized by Medicare and link to their services. Additionally you can contact Medicare directly.
My hope is that by arming people with a few key questions and more information, we can help them make a seamless and stress free switch to a provider they trust. In that way, they will be able to rest assured after July 1 that their supplies will be waiting for them in the mailbox, just as always.
Terry Blankenship is vice president of patient care at Diabetes Care Club, the nation’s 3rd largest provider of diabetic testing supplies and one of only 18 companies authorized to serve Medicare patients. He invites people to email questions to tblankenship@simplexhealthcare.com. For further information on Diabetes Care Club, visit www.diabetescareclub.com. Or call 1-800-376-7521.


 pre-diabetes.
pre-diabetes.